Love this pharmacy vending machine at USC! No GYNO crap to be found!
Instead, birth control pills, plan B, condoms, tampons, COVID tests, and hydrocortisone (the thing to use in a pinch for a bad vulvar itch instead of Vagisil, the devil’s own sav. (Vagisil has benzocaine and this can cause allergic reactions and irritation. And we hate Vagisil because of they are a massive part of the feminine hygiene industry invested in the messaging that women smell).
Love this pharmacy vending machine at USC! No GYNO crap to be found!
Instead, birth control pills, plan B, condoms, tampons, COVID tests, and hydrocortisone (the thing to use in a pinch for a bad vulvar itch instead of Vagisil, the devil’s own sav. (Vagisil has benzocaine and this can cause allergic reactions and irritation. And we hate Vagisil because of they are a massive part of the feminine hygiene industry invested in the messaging that women smell).
Love this pharmacy vending machine at USC! No GYNO crap to be found!
Instead, birth control pills, plan B, condoms, tampons, COVID tests, and hydrocortisone (the thing to use in a pinch for a bad vulvar itch instead of Vagisil, the devil’s own sav. (Vagisil has benzocaine and this can cause allergic reactions and irritation. And we hate Vagisil because of they are a massive part of the feminine hygiene industry invested in the messaging that women smell).
Love this pharmacy vending machine at USC! No GYNO crap to be found!
Instead, birth control pills, plan B, condoms, tampons, COVID tests, and hydrocortisone (the thing to use in a pinch for a bad vulvar itch instead of Vagisil, the devil’s own sav. (Vagisil has benzocaine and this can cause allergic reactions and irritation. And we hate Vagisil because of they are a massive part of the feminine hygiene industry invested in the messaging that women smell).
Love this pharmacy vending machine at USC! No GYNO crap to be found!
Instead, birth control pills, plan B, condoms, tampons, COVID tests, and hydrocortisone (the thing to use in a pinch for a bad vulvar itch instead of Vagisil, the devil’s own sav. (Vagisil has benzocaine and this can cause allergic reactions and irritation. And we hate Vagisil because of they are a massive part of the feminine hygiene industry invested in the messaging that women smell).
I made the mistake of accidentally googling myself…
Calling out people who sell unregulated, untested pharmaceuticals (supplements with health claims, not products like prenatal vitamins or iron for iron deficiency) seems to get people mad. Like really mad. I’ve been doing this for ages (hello GOOP) and have been pretty vocal about how these people are making money hand over fist for products that are not recommended in guidelines and often have little to no (it is usually no) data to support their use. Remember, if the data were good they would be in the guidelines! Whether it is a company, celebrity, medical doctor, naturopath, chiropractor, PhD, nurse…ok you get the picture…doesn’t matter. It irks me to no end that people give their heard earned money for false promises…false promises that may also net them liver injury to boot. So why now all of a sudden people are hot about it is fascinating to me. I’ve called out numerous prenatal vitamins, the liver shield, menopause supplements, probiotics etc. I have some theories, and I’m sure I will write about it at some point.
Thinking I’m mean, the person not making money from supplements, for pointing out the dismal research, safety issues, and overall grift is a weird flex. No one likes to be led astray. But really, shouldn’t the anger be directed at the people making tens or hundreds of thousands or even millions of dollars from selling products with dismal data?
Being appropriately confident is just that. And I’m not going to lie to you to oversell things for attention. Women’s health has too long been a pendulum where something is new and amazing or essential and pushed on everyone or it’s the opposite. I want to help women with data and, when that is absent, experience, not trends. Because that is the kind of care that I want.
I’m not looking for anything in reply. But if you are hate following me, maybe reconsider. Life is too short for that. And please don’t go looking for the sub-Reddit. I just found the 3 buckets really fascinating, and I bet some of you will as well!
Also, it has just spurred me on to write about more supplements!
As you were!
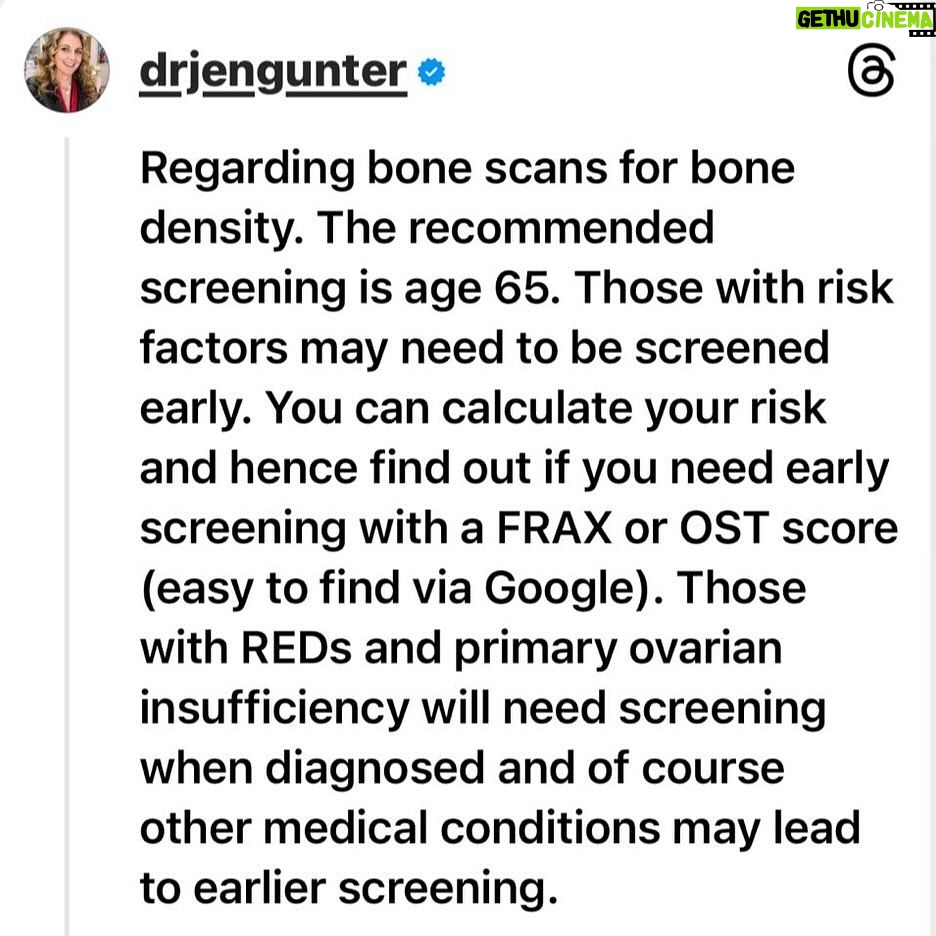
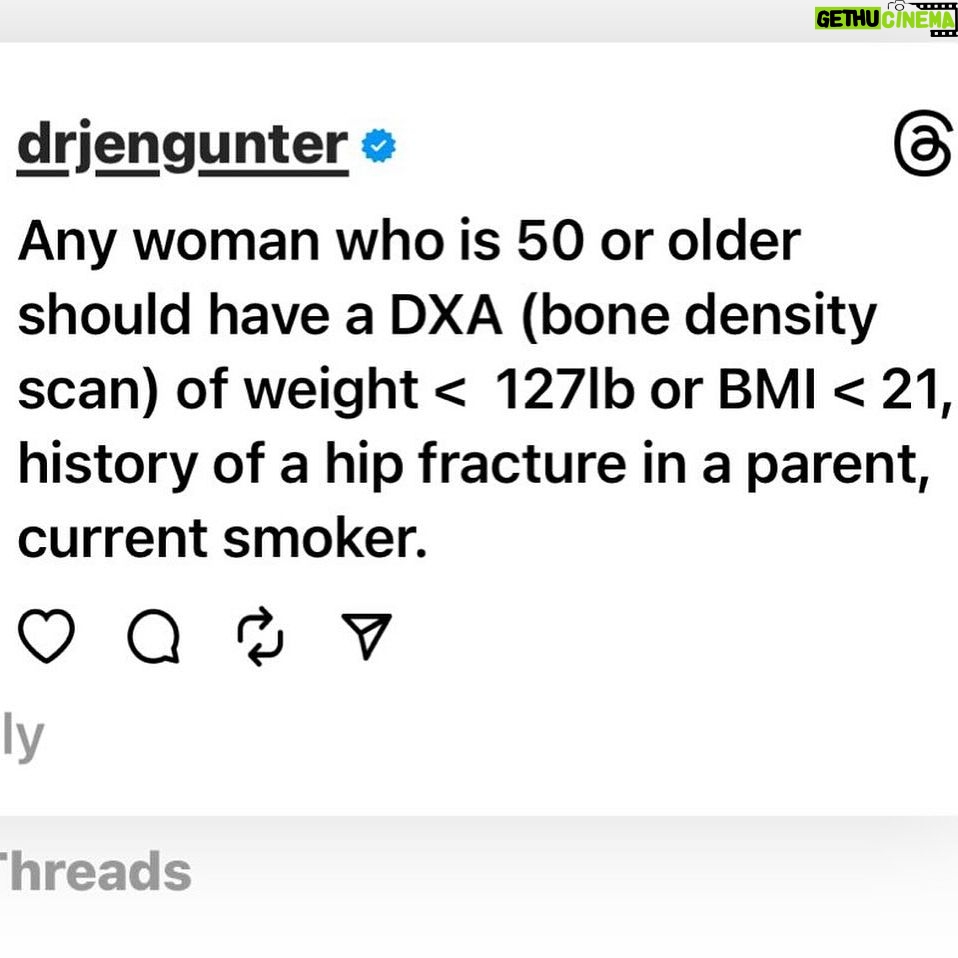
Thought I would share this bone density screening info that I posted on threads. It seems there are people recommending baseline DXA (bone density) scans for all women in their 30s and 40s, but screening under age 65 is risk based.
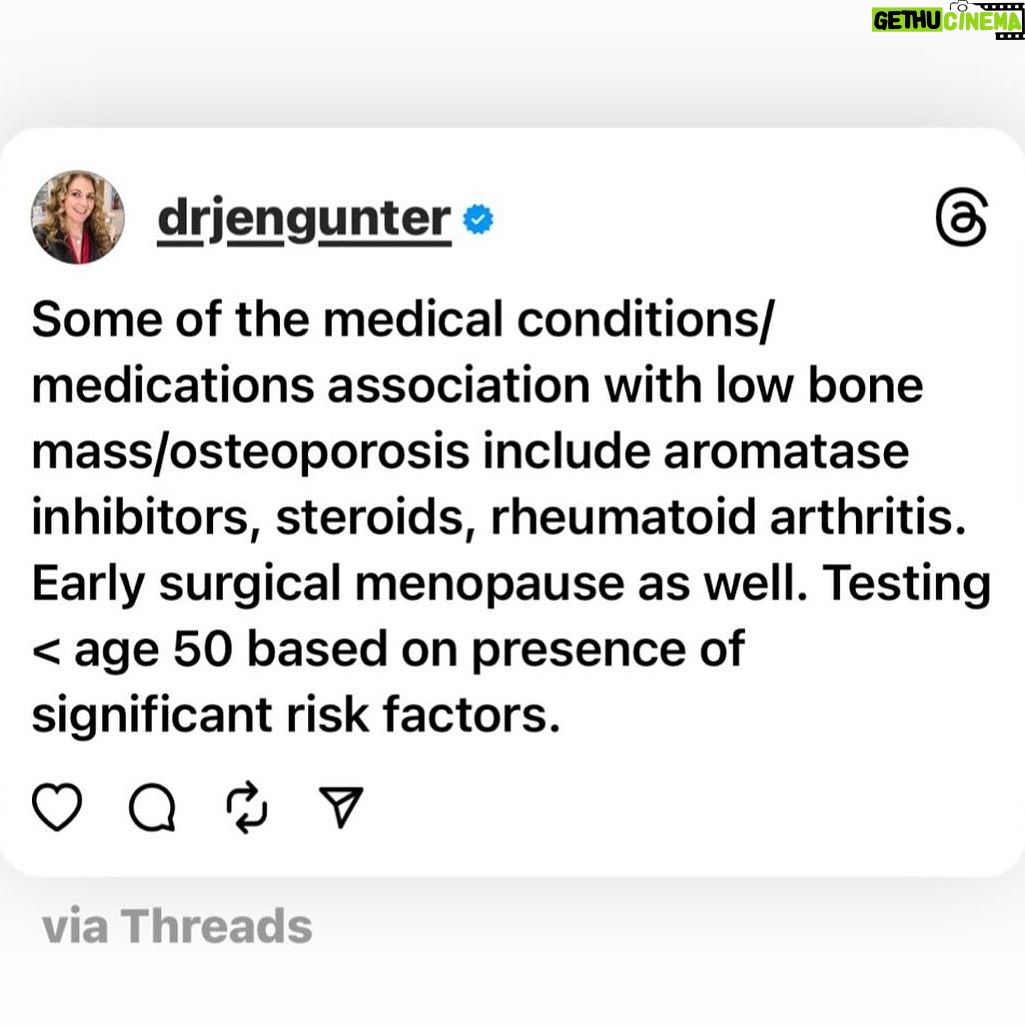
For people age 50 and older we screen earlier than 65 based on weight, history of parental hip fracture, and if someone smokes. There are other risk factors to include as well, and a variety of medical conditions and medications that would promote earlier screening. For example, anyone with primary ovarian insufficiency should get a bone scan when they are diagnosed as should people with relative energy deficiency of sports (REDs).
When to screen under age 50 depends primarily on risk factors.
Other tools to help determine risk and if you ahold be screened earlier are FRAX and OST and if you Google them, you should find the calculators.
For people with no risk factors, screening earlier isn’t recommended.
Thought I would share this bone density screening info that I posted on threads. It seems there are people recommending baseline DXA (bone density) scans for all women in their 30s and 40s, but screening under age 65 is risk based.
For people age 50 and older we screen earlier than 65 based on weight, history of parental hip fracture, and if someone smokes. There are other risk factors to include as well, and a variety of medical conditions and medications that would promote earlier screening. For example, anyone with primary ovarian insufficiency should get a bone scan when they are diagnosed as should people with relative energy deficiency of sports (REDs).
When to screen under age 50 depends primarily on risk factors.
Other tools to help determine risk and if you ahold be screened earlier are FRAX and OST and if you Google them, you should find the calculators.
For people with no risk factors, screening earlier isn’t recommended.
Thought I would share this bone density screening info that I posted on threads. It seems there are people recommending baseline DXA (bone density) scans for all women in their 30s and 40s, but screening under age 65 is risk based.
For people age 50 and older we screen earlier than 65 based on weight, history of parental hip fracture, and if someone smokes. There are other risk factors to include as well, and a variety of medical conditions and medications that would promote earlier screening. For example, anyone with primary ovarian insufficiency should get a bone scan when they are diagnosed as should people with relative energy deficiency of sports (REDs).
When to screen under age 50 depends primarily on risk factors.
Other tools to help determine risk and if you ahold be screened earlier are FRAX and OST and if you Google them, you should find the calculators.
For people with no risk factors, screening earlier isn’t recommended.
Thought I would share this bone density screening info that I posted on threads. It seems there are people recommending baseline DXA (bone density) scans for all women in their 30s and 40s, but screening under age 65 is risk based.
For people age 50 and older we screen earlier than 65 based on weight, history of parental hip fracture, and if someone smokes. There are other risk factors to include as well, and a variety of medical conditions and medications that would promote earlier screening. For example, anyone with primary ovarian insufficiency should get a bone scan when they are diagnosed as should people with relative energy deficiency of sports (REDs).
When to screen under age 50 depends primarily on risk factors.
Other tools to help determine risk and if you ahold be screened earlier are FRAX and OST and if you Google them, you should find the calculators.
For people with no risk factors, screening earlier isn’t recommended.
I wrote about the new study looking at the use of hormone therapy for those age 65 and older. This is not starting therapy, but continuing. It is an observational study, so has limitations. Here’s a summary for the estrogen only portion. This does not apply to estrogen plus a progestogen, I will cover that part in another post. My full write up is at TheVajenda.com where you will find a lot more detail.
****
In most cases the best outcomes were seen with transdermal or vaginal therapy and at lower or medium doses. One exception is oral Premarin and breast cancer.
All the estrogens reduced mortality, with estradiol at 21%, which was better than Premarin at 13%.
With breast cancer, had the greatest benefit with a 23% reduction. However, transdermal estradiol was associated with a 14% reduction in breast cancer risk. As expected, low-dose vaginal estrogen, which should not be absorbed, was neutral from a breast cancer reduction perspective. Colon and lung cancer reduction was fairly similar across all the estrogens. The reduction in lung cancer with low-dose vaginal estrogen doesn’t seem biologically plausible!
Improvement in heart disease was less certain, but a positive trend was seen with lower doses and transdermal/vaginal.
Reduction in dementia was only seen with low dose transdermal. Would not draw any grand conclusions about dementia.
There were some issues, specifically some unexplainable health benefits were seen with low dose vaginal estrogen, which sometimes performed better than transdermal estrogen which seems biologically implausible. This suggests there may be some biases we don’t know about and I would causation people from jumping to conclusions about using this study to start therapy, otherwise you are going to have to explain how low dose vaginal estradiol tablets and the estradiol ring reduce lung cancer!
Overall, there were no concerning safety signals, and that is reassuring. So the idea that women are increasing their risk of breast cancer, heart disease, or dementia by staying on estrogen therapy over age 65 isn’t supported by this study. Stay tuned for my write up on the estrogen and progestogen part of the study.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Lots of questions about testosterone lately and I am not sure why, but because of these I wrote a very detailed post for The Vajenda last week.
I have included several slides summarizing the Global Consensus Statement on the Use of Testosterone for Women and a summary of the British Menopause Society recommendations. If the data is there to support testosterone for many reasons outside of low libido, why can’t any menopause of endocrine society find it? I also included a slide with the organizations that signed off on the statement.
Here is the summary from my piece. Head to The Vajenda if you want the whole piece or the references:
✅ Testosterone levels gradually decrease throughout a woman’s lifetime. There is no sharp drop around menopause.
🤝The majority of testosterone is bound to carrier proteins, but we still don’t really understand what that means regarding testosterone’s impact on the body.
🏭Testosterone has a significant intracrinology, meaning it is also made inside cells, so testosterone levels really do not tell us the whole picture.
✅Checking testosterone for well-being or symptoms of menopause is unhelpful and a waste of your hard-earned money.
❓Testosterone levels don’t predict symptoms.
📊Current studies do not support the use of testosterone for ANY reason outside of treating libido. This includes muscle mass and protecting bone health.
📑Studies with primary ovarian insufficiency don’t show an added benefit from testosterone.
💪Improvement in muscle mass/strength likely only occurs when testosterone levels are much higher than normal.
Son who is back from college wanted homemade bagels. I asked if he could wait 3 ish hours? And he could.
Very tasty! Not that much effort. Made the dough. Went to the store while it proofed and to get some lox.
Then boiled and baked!
Recipe is from the always amazing @sallysbakeblog
Son who is back from college wanted homemade bagels. I asked if he could wait 3 ish hours? And he could.
Very tasty! Not that much effort. Made the dough. Went to the store while it proofed and to get some lox.
Then boiled and baked!
Recipe is from the always amazing @sallysbakeblog
It was a day of baking! Cheesecake with strawberry sauce. No cracks in the cheesecake!!!!
Also a @sallysbakeblog recipe. I have made it several times and it is soooooo tasty.
It was a day of baking! Cheesecake with strawberry sauce. No cracks in the cheesecake!!!!
Also a @sallysbakeblog recipe. I have made it several times and it is soooooo tasty.
Pleasantly surprised to find out that Blood: The Science, Medicine, and Mythology of Menstruation is one of the most popular nonfiction books on @goodreads so far for 2024.
I was surprised because my books always get some purposely awful reviews from the unregulated, unstudied pharmaceutical industry, a.k.a. those who support naturopaths, functional providers or all kinds, and the wellness industrial complex. To be clear, I review the evidence, such as it is, for many “natural” products in this book and it is patriarchal to say women should follow practices and therapies with essentially zero quality research! Don’t women deserve research? 🧐 it’s not my fault the studies are crap and the unscrupulous have no issue with that! I discuss a variety of different supplements in the book and present the research such as it is so people can make informed choices.
I get questions in my DMs constantly, and almost always you can find the answer in Blood, one of my other books, or on The Vajenda! For example, this week I was asked about CBD tampons (info is in Blood), what to do when you are in your 20s and have not had a period in 4 months (answer in Blood), and what do I think of supplements for PMS (also in Blood!).
Thank you to everyone who read Blood and reviewed it. It means a lot of me.
Pleasantly surprised to find out that Blood: The Science, Medicine, and Mythology of Menstruation is one of the most popular nonfiction books on @goodreads so far for 2024.
I was surprised because my books always get some purposely awful reviews from the unregulated, unstudied pharmaceutical industry, a.k.a. those who support naturopaths, functional providers or all kinds, and the wellness industrial complex. To be clear, I review the evidence, such as it is, for many “natural” products in this book and it is patriarchal to say women should follow practices and therapies with essentially zero quality research! Don’t women deserve research? 🧐 it’s not my fault the studies are crap and the unscrupulous have no issue with that! I discuss a variety of different supplements in the book and present the research such as it is so people can make informed choices.
I get questions in my DMs constantly, and almost always you can find the answer in Blood, one of my other books, or on The Vajenda! For example, this week I was asked about CBD tampons (info is in Blood), what to do when you are in your 20s and have not had a period in 4 months (answer in Blood), and what do I think of supplements for PMS (also in Blood!).
Thank you to everyone who read Blood and reviewed it. It means a lot of me.
Pleasantly surprised to find out that Blood: The Science, Medicine, and Mythology of Menstruation is one of the most popular nonfiction books on @goodreads so far for 2024.
I was surprised because my books always get some purposely awful reviews from the unregulated, unstudied pharmaceutical industry, a.k.a. those who support naturopaths, functional providers or all kinds, and the wellness industrial complex. To be clear, I review the evidence, such as it is, for many “natural” products in this book and it is patriarchal to say women should follow practices and therapies with essentially zero quality research! Don’t women deserve research? 🧐 it’s not my fault the studies are crap and the unscrupulous have no issue with that! I discuss a variety of different supplements in the book and present the research such as it is so people can make informed choices.
I get questions in my DMs constantly, and almost always you can find the answer in Blood, one of my other books, or on The Vajenda! For example, this week I was asked about CBD tampons (info is in Blood), what to do when you are in your 20s and have not had a period in 4 months (answer in Blood), and what do I think of supplements for PMS (also in Blood!).
Thank you to everyone who read Blood and reviewed it. It means a lot of me.

{kind=link}